How Do You Know You Have Lymphedema? Signs, Symptoms, and What to Do Next

If your leg feels like it's packed with cement, or one arm looks noticeably larger than the other, something is happening beneath the surface that your body is trying to tell you. Maybe the swelling comes and goes. Maybe it has been building slowly for months. Maybe a doctor mentioned the word "lymphedema" at a follow-up after surgery or cancer treatment and you weren't sure what to make of it.
This guide is written for patients and caregivers who want straight answers — whether you have a confirmed diagnosis, a suspicion, or simply persistent swelling that hasn't been explained. By the end, you will understand exactly what lymphedema is, how to recognize its key warning signs, how to tell it apart from ordinary water retention, why it develops, and most importantly — what to do next.
What Is Lymphedema? A Clear Definition
Lymphedema is the chronic accumulation of protein-rich fluid in the body's soft tissues, caused by damage to or dysfunction of the lymphatic system.
According to the Mayo Clinic, lymphedema most commonly affects the arms or legs, though it can also occur in the chest wall, abdomen, neck, and genitals. It is not a cosmetic condition and it does not resolve on its own. Without proper management, it is progressive — meaning it advances through stages that become increasingly difficult to treat.
The key point: lymphedema is not the same as ordinary swelling. It is a recognized chronic medical condition with a specific cause, a specific mechanism, and a specific treatment approach. Understanding that distinction is the first step toward getting the right care.
The Lymphatic System: Your Body's Hidden Pump
To understand lymphedema, you need to understand what the lymphatic system actually does — because most patients were never taught.
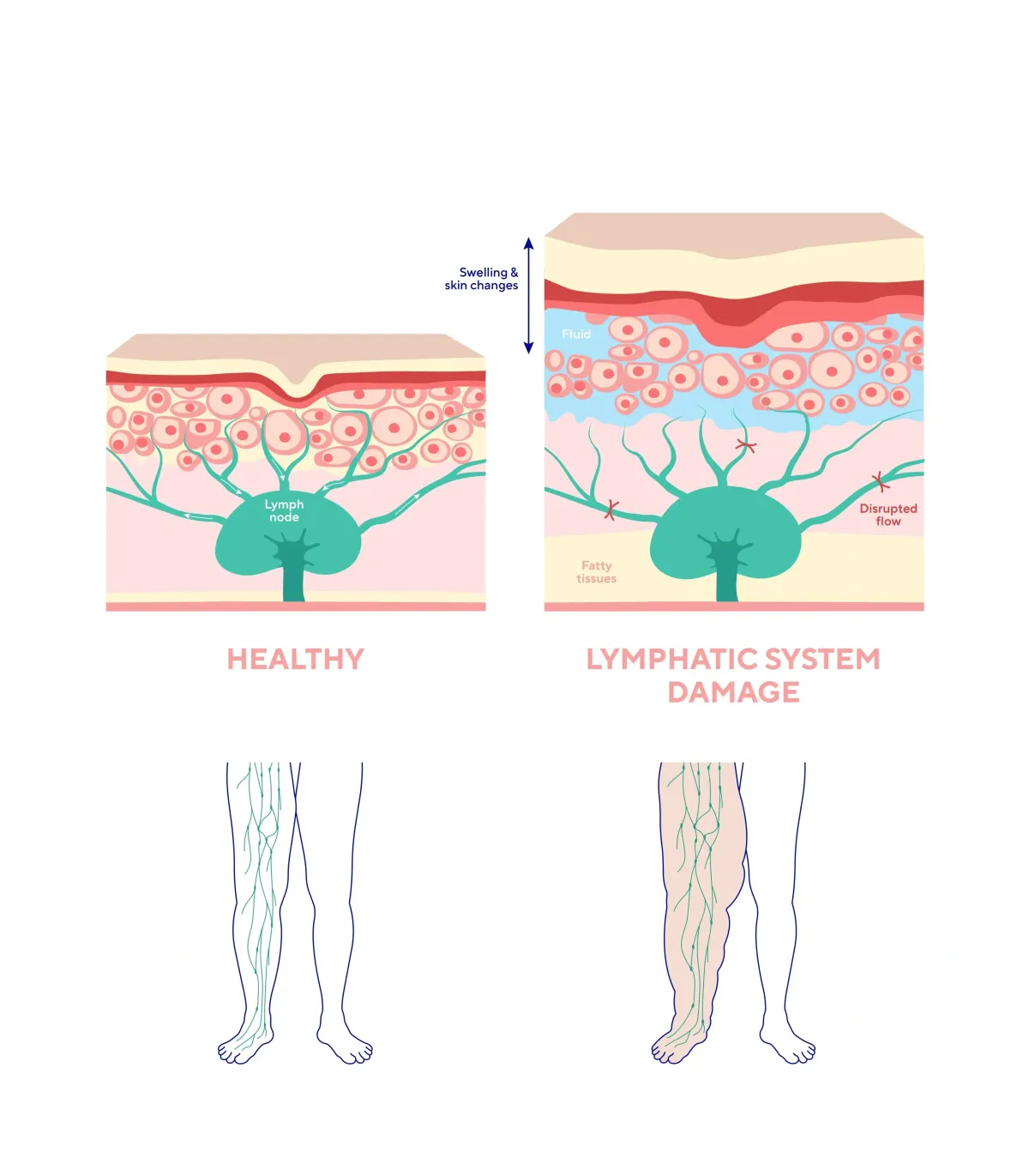
Think of your lymph nodes as pumps. Positioned throughout your body — in your neck, armpits, groin, chest, and abdomen — their job is to circulate lymphatic fluid through a vast network of vessels. This fluid does far more than drain waste. It carries white blood cells, nutrients, and immune factors that actively feed and protect your tissues. Lymph nodes are not passive filters. They are active participants in your immune system.
When lymph nodes are damaged, surgically removed, or overwhelmed by chronic illness, this circulation slows or stops. Fluid backs up in the tissue. The affected limb swells. The immune function in that region weakens. And without treatment, the accumulated protein-rich fluid triggers inflammation and eventually causes the tissue itself to harden — a process called fibrosis that makes the condition progressively more difficult to reverse.
This is why lymphedema is a whole-body problem, not just a nuisance.
Key Warning Signs: How Do You Know You Have Lymphedema?
Sign 1: Your Limb Feels Hard as a Rock
One of the most telling differences between lymphedema and general swelling is what the tissue feels like under your hand.
In normal or mildly swollen tissue, there is pliability — a softness that gives under pressure. With lymphedema, particularly as it advances, the limb begins to feel dense, firm, and increasingly hard. Patients describe it as a limb packed with something solid, or skin stretched tight that doesn't give the way it should.
This happens because lymphatic fluid is protein-rich. When it stagnates in tissue over time, it initiates fibrosis — the deposition of fibrous connective tissue that progressively stiffens the affected area. Research published on PubMed explains that when lymphatic vessels are damaged, increased pressure weakens the junctions between lymphatic endothelial cells, causing lymph leakage and fluid stasis that activates inflammatory cells responsible for producing fibrotic tissue. Early-stage lymphedema may still feel soft and squishy. Late-stage lymphedema can feel woody or leathery.
If your limb feels abnormally firm — especially when elevation brings no relief — that is a red flag requiring medical evaluation.
Sign 2: The "Bounce Back" Test — Pitting Edema
Here is a simple, at-home observation that clinicians use as an initial indicator:
Press your thumb firmly into the swollen area for 5 to 10 seconds. Then release. Watch what happens.
In temporary fluid retention, the tissue rebounds quickly — typically within one to two seconds. In lymphedema, the indentation (called a "pit") remains. The tissue is slow to return, or doesn't return at all. This is called pitting edema, and the speed of bounce-back tells a meaningful clinical story.
Fast bounce-back (1–2 seconds): More consistent with mild, temporary fluid retention
Slow bounce-back (5–30+ seconds): Consistent with significant edema, possibly lymphedema
No bounce-back, tissue feels firm: May indicate more advanced lymphedema with fibrosis
Clinical staging of lymphedema recognizes that in Stage 1, pressing on the swelling leaves an indentation that doesn't automatically spring back — this is pitting edema — and the puffiness may reduce with elevation. By Stage 2, the swelling no longer resolves with elevation and the skin begins to feel tougher.
This test is not a diagnosis. But it is valuable information to bring to your doctor. Note how long recovery takes, which limb is affected, and whether both sides respond the same way.
Sign 3: Swelling That Does Not Resolve Overnight
Ordinary water retention from a long flight, a salty meal, or hours on your feet typically responds to rest and elevation. Prop your legs up and the swelling is meaningfully improved by morning.
Lymphedema does not follow this pattern. Many patients wake up with a limb still significantly swollen, and by afternoon it is worse again. Elevation may provide modest early relief in Stage 1, but it does not produce the consistent improvement you would see with simple fluid retention. This persistence — swelling that elevation doesn't resolve — is one of the hallmarks that distinguishes lymphedema from other causes of edema.
Sign 4: Asymmetric Swelling — One Side Significantly Larger
Bilateral swelling affecting both legs or both arms equally tends to suggest systemic causes — heart failure, kidney disease, or venous insufficiency. Lymphedema, especially in earlier stages, is frequently unilateral: one limb noticeably larger, heavier, or tighter than the other.
If your pants feel different on each leg, if a ring only feels tight on one hand, if one arm feels noticeably heavier during daily tasks — that asymmetry is worth documenting. Take photos with a date stamp. Note measurements if possible. Bring that information to your physician.
Sign 5: Heaviness, Tightness, and Aching
Lymphedema is not always acutely painful, but it produces a consistent set of sensations that patients describe in similar ways:
Heaviness: The limb feels weighted, as if gravity is pulling it harder than usual
Tightness: Clothing, shoes, or jewelry feel constricting on the affected side, even when sized correctly
Aching: A dull, persistent fatigue in the limb that worsens as the day progresses or after activity
Reduced range of motion: Difficulty fully bending or extending the affected knee, elbow, wrist, or ankle
These are early warning signals. The National Lymphedema Network emphasizes that screening and early detection — catching these signs before advanced swelling sets in — gives patients dramatically better outcomes than waiting until the condition is visibly severe.

Lymphedema vs. Water Retention: How to Tell the Difference
This is the most common source of confusion — and one of the most important distinctions to make, because the treatment approaches are fundamentally different.
Water Retention (General Edema)
Typically affects both limbs relatively equally
Responds to elevation, reduced sodium intake, and sometimes diuretics
Often triggered by prolonged sitting, heat, hormonal shifts, or dietary factors
Pitting edema may be present but resolves quickly
Comes and goes without progressive tissue changes
Lymphedema
Frequently unilateral, particularly in earlier stages
Does not respond adequately to diuretics alone — and long-term diuretic use can concentrate the protein in stagnant lymphatic fluid, worsening fibrotic tissue changes over time
Persistent and progressive without specialized lymphedema treatment
Requires complete decongestive therapy, properly fitted compression garments, and in many cases a lymphedema pump
Caused by structural damage or dysfunction of the lymphatic system
Poor Circulation and Venous Insufficiency
There is a third category that often overlaps with lymphedema: chronic venous insufficiency (CVI), where the leg veins struggle to return blood efficiently to the heart. According to NIH's StatPearls, nononcologic causes of lymphedema include chronic venous insufficiency alongside trauma and inflammatory conditions. In practice, the two conditions frequently coexist — a combination called phlebolymphedema. Poor venous return increases the fluid burden on the lymphatic system; when that system is already compromised, both worsen together. Skin discoloration, varicose veins, ankle thickening, or leg ulcers alongside persistent swelling suggest both systems need evaluation.
The CDC's lymphedema and cancer resource and the American Cancer Society's lymphedema treatment guide both note that distinguishing lymphedema from other causes of swelling is essential to receiving the right treatment — reinforcing why a physician evaluation is always the necessary first step.
Who Gets Lymphedema? The Most Common Causes
Lymphedema doesn't appear without cause. In virtually every case there is an underlying medical reason — which is why the most important first step is always talking to your doctor. Here are the most common contributors seen in clinical practice.
Cancer and Cancer Treatment
The most recognized cause of secondary lymphedema in the United States is lymph node removal or radiation as part of cancer treatment. Mayo Clinic reports that approximately 40% of people who undergo breast cancer surgery involving lymph node removal will develop lymphedema. The same risk applies — at varying rates — to patients treated for prostate, bladder, gynecologic, colorectal, and head and neck cancers. Importantly, lymphedema may not appear until months or even years after treatment ends.
Diabetes
Diabetes damages peripheral nerves and blood vessels, impairs wound healing, and contributes to chronic lower extremity swelling. Diabetic patients face compounding risk from both venous insufficiency and compromised lymphatic function. If you are managing diabetes and noticing persistent leg swelling, our team works closely with diabetic patients to provide appropriate compression and footwear support alongside your medical care.
Obesity
Research published in PubMed has established that extreme obesity can independently cause lower extremity lymphedema — termed obesity-induced lymphedema — with risk increasing significantly once BMI exceeds 40, and becoming nearly universal when BMI exceeds 60. Excess body weight places mechanical pressure on lymphatic vessels, impairs their pumping capacity, and creates a self-reinforcing cycle of fluid accumulation, adipose deposition, and further lymphatic damage.
COPD
Patients with advanced chronic obstructive pulmonary disease develop elevated thoracic pressure and reduced cardiac efficiency that can impair lymphatic drainage from the lower extremities. Persistent lower leg swelling in COPD patients warrants evaluation for a lymphatic component alongside cardiac and pulmonary causes.
Renal Failure
When kidney function declines, the body's ability to regulate fluid balance is compromised systemically. The resulting fluid overload can overwhelm the lymphatic system, producing swelling that shares characteristics with lymphedema even when the primary mechanism is renal rather than purely lymphatic.
Cardiac Surgery — Especially CABG
This is one of the most underrecognized causes of secondary lymphedema, and one worth knowing. A case report and literature review published in PMC documents that secondary lymphedema can develop after saphenous vein harvesting for coronary artery bypass graft surgery, with the condition sometimes presenting a decade or more after the procedure. The saphenous vein runs alongside important lymphatic channels in the leg; when it is harvested for bypass surgery, those channels are disrupted. Patients who have had CABG and notice progressive leg swelling on the harvest side should specifically mention this surgical history to their physician.
Other Surgical Consequences
Any procedure involving the pelvis, abdomen, groin, or lymph node regions — including hip replacement, hernia repair, vascular surgery, and gynecologic procedures — carries some risk of disrupting lymphatic pathways and triggering secondary lymphedema.

Expert Insights: What Clinicians Want You to Know
Early Intervention Produces Dramatically Better Outcomes
Lymphedema does not get better on its own. Clinical staging shows that early-stage lymphedema — where pitting edema is still present and elevation provides some relief — is far more responsive to treatment than advanced stages where swelling becomes permanent, the skin hardens, and fluid may begin leaking directly from the skin surface. The earlier lymphedema is identified and properly managed, the more effectively it can be controlled.
If you are experiencing swelling, heaviness, or asymmetry — especially with any of the risk factors described above — do not wait for it to become a crisis. Ask your physician for a referral to a certified lymphedema therapist (CLT).
Compression Is the Foundation of Management
Once lymphedema is diagnosed, compression therapy is the primary management tool. Properly fitted gradient compression garments — stockings, arm sleeves, gauntlets, or wraps — provide external pressure that helps the lymphatic system move fluid more efficiently by compensating for its damaged internal mechanism.
Fit matters enormously. Poorly fitted garments create pressure gradients in the wrong direction and can worsen the condition. At MCB DME, we specialize in fitting patients with clinically appropriate compression garments based on limb measurements, diagnosis, and lifestyle — not off-the-shelf guesswork.
Pneumatic Compression Devices Can Help When Indicated
For patients with moderate to severe lymphedema, a pneumatic compression pump provides mechanical assistance by sequentially inflating air chambers from the extremity toward the core, mimicking the natural pumping action that damaged lymph nodes can no longer provide. These devices are covered by Medicare and most commercial insurance plans when properly prescribed and documented. Our team handles the verification and authorization process so patients can focus on their care.
Diuretics Alone Are Not the Answer
A common clinical mistake — and a significant source of patient frustration — is treating lymphedema with diuretics alone. While diuretics reduce overall fluid volume, they do not address the underlying lymphatic dysfunction. Worse, by drawing water out of the tissue while leaving protein-rich lymph fluid behind, long-term diuretic use can increase the protein concentration in the affected tissue, accelerating the fibrotic changes that make lymphedema harder to treat. Compression therapy and manual lymphatic drainage are the evidence-based cornerstones of treatment, not diuretics.
Always Ask Your Doctor First
Swelling in a limb can have multiple causes — including deep vein thrombosis, infection, tumor, or cardiac causes — some of which require urgent medical attention. Never self-diagnose lymphedema. Use this guide to recognize warning signs, gather observations, and have an informed conversation with your physician. Your doctor can examine you, order appropriate imaging, and coordinate a treatment plan that addresses the actual cause.
Common Mistakes and Misconceptions
"It's just normal swelling — I'll wait it out." Lymphedema is progressive. Stage 1 is dramatically easier to treat than Stage 3. Waiting makes the outcome worse, not better.
"Diuretics will fix it." Diuretics address fluid volume but not lymphatic dysfunction. Used alone for lymphedema, they can worsen fibrotic changes over time.
"My swelling goes down overnight, so it can't be lymphedema." Early-stage lymphedema may partially respond to elevation. That doesn't rule it out — it may simply mean you're in an earlier, more treatable stage.
"Lymphedema only happens to cancer patients." While cancer treatment is a leading cause, millions of Americans develop lymphedema through diabetes, obesity, cardiac surgery, COPD, renal failure, and other non-oncologic pathways.
"There's nothing you can do about it." Lymphedema has no cure, but it is highly manageable. Most patients who receive appropriate treatment — compression therapy, manual lymphatic drainage, pump therapy, and proper DME — experience significant reduction in symptoms and prevention of progression. Our providers page outlines how MCB DME partners with clinical teams to coordinate that care.

Frequently Asked Questions About Lymphedema
What does lymphedema feel like at first?
Before visible swelling appears, most patients notice that a limb feels heavier, tighter, or fatigues more quickly than usual. Clothing or jewelry may feel subtly different on one side. These early sensory changes — before the limb looks obviously swollen — are often the first sign that lymphatic drainage is being compromised.
Is lymphedema the same as water retention?
No. Water retention (general edema) results from temporary fluid imbalance and typically resolves with elevation, rest, or dietary adjustments. Lymphedema results from structural damage to the lymphatic system and does not resolve on its own. The treatments are different, and applying general edema management to lymphedema — particularly diuretics — can make the condition worse over time.
How is lymphedema diagnosed?
Diagnosis is made clinically by a physician through examination and patient history. Imaging studies such as lymphoscintigraphy or MRI may be used to confirm the diagnosis or assess severity. There is no simple blood test. If lymphedema is suspected, your doctor may refer you to a vascular specialist or a certified lymphedema therapist for further evaluation. The National Lymphedema Network's diagnosis and imaging page provides a helpful overview of what that evaluation involves.
Can lymphedema go away on its own?
No. Lymphedema results from damage to the lymphatic system's structure. Without treatment, it will progress through increasingly advanced stages. With appropriate, consistent treatment — compression, manual lymphatic drainage, pump therapy, and skin care — most patients can significantly reduce symptoms and stabilize the condition.
What is the difference between pitting and non-pitting edema?
Pitting edema leaves a visible indentation when pressed — the tissue is slow to rebound. Non-pitting edema does not leave an indentation; the tissue feels firmer or rubbery. Early lymphedema typically causes pitting edema. As fibrosis develops in later stages, the edema may become non-pitting, reflecting permanent structural changes in the tissue.
Does insurance cover lymphedema treatment?
Medicare and most commercial insurance plans cover medically necessary lymphedema treatment including compression garments and pneumatic compression devices when properly prescribed and documented. Coverage varies by plan. MCB DME verifies your benefits, manages the authorization process, and handles billing directly. Contact our patient support team for a free benefits check.
What should I do if I think I have lymphedema?
Schedule an appointment with your primary care physician or specialist as soon as possible. Describe your symptoms in detail — when the swelling began, which limb is affected, how it responds to elevation, and your full medical and surgical history. Bring photos if swelling is intermittent. Ask for a referral to a certified lymphedema therapist or vascular specialist. The sooner a diagnosis is confirmed, the more treatment options are available to you.
Is lymphedema dangerous?
Lymphedema itself is chronic but not immediately life-threatening. However, it creates serious secondary risks. Mayo Clinic notes that severe lymphedema can affect the ability to move the affected limb, significantly increases the risk of skin infections and sepsis, and can lead to progressive skin changes and breakdown. Mayo ClinicThe National Lymphedema Network's page on infections and complications outlines these risks in detail and emphasizes why ongoing management — not just initial treatment — is essential.
When to Seek Immediate Medical Attention
While lymphedema typically develops gradually, certain signs require prompt or emergency evaluation:
Sudden, severe swelling in one limb — could indicate deep vein thrombosis (DVT), a medical emergency
Red streaking, warmth, fever alongside swelling — signs of cellulitis or lymphangitis, infections that can spread rapidly
Chest pain or shortness of breath with leg swelling — possible pulmonary embolism
Rapidly worsening swelling with no clear explanation — needs same-day evaluation
Do not attempt to diagnose yourself in these situations. Contact your physician immediately or go to the emergency room.
Key Takeaways
Lymphedema is swelling caused by damage to the lymphatic system — not ordinary water retention, and not something that resolves on its own
Key warning signs include a limb that feels abnormally firm or hard, slow or absent "bounce-back" when pressed, persistent unilateral swelling, and heaviness or tightness in the affected limb
The at-home pitting edema test (press and release) is a useful observation — but a physician must confirm the diagnosis
Lymph nodes are your body's fluid pumps — when they are removed, damaged, or overwhelmed, fluid accumulates and immune function in the area declines
Lymphedema most commonly follows cancer treatment, diabetes, obesity, COPD, renal failure, or surgery — especially CABG with saphenous vein harvesting
Diuretics alone are not an effective treatment and can worsen lymphedema over time
Early intervention produces dramatically better outcomes than waiting
Compression garments, manual lymphatic drainage, and pneumatic pump therapy are the cornerstones of management
Next Steps: How MCB DME Can Help
If you or someone you care for is experiencing symptoms that may indicate lymphedema, the first step is always a conversation with your doctor. Once a diagnosis is confirmed, MCB DME is here to support every aspect of your equipment needs.
We are a Hawthorne, New Jersey-based durable medical equipment provider specializing in:
Lymphedema pumps — pneumatic compression devices covered by Medicare and most insurance plans
Compression garments — properly measured and fitted stockings, sleeves, and wraps for lymphedema management
Diabetic and orthopedic footwear — for patients managing diabetes alongside lymphedema
Arterial compression therapy — for patients with peripheral arterial disease or poor lower limb circulation
Bracing and orthopedic support — for musculoskeletal conditions that accompany chronic illness
Insurance verification and billing — we handle the paperwork so you don't have to
For physicians, wound care nurses, and care coordinators, visit our providers page to learn how we support clinical teams and streamline equipment authorization. For patients ready to get started, our patients page outlines exactly what to expect. Or call us directly at (973) 553-0777 — our team is here to help.
Related Topics You May Find Helpful
What Is Lymphedema and Why Do I Have It: A Comprehensive Guide to Understanding Your Diagnosis
Flat Knit vs. Circular Knit Compression Garments: How to Choose
Lymphedema Diet Guide: Anti-Inflammatory Foods & Nutrition Tips
About MCB DME
MCB DME is a durable medical equipment provider based in Hawthorne, New Jersey, dedicated to improving patient outcomes through clinically appropriate, insurance-covered medical equipment. We specialize in lymphedema management, compression therapy, diabetic footwear, arterial pumps, bracing, and prosthetics — serving patients and healthcare providers throughout New Jersey. Our team handles insurance verification, prior authorizations, and billing directly, so patients can focus on their health rather than the paperwork.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.
