Vascular Wounds and Arterial Wounds: Compression Therapy, Pumps, and Proper Care
Quick Answer: Vascular wounds are chronic wounds caused by impaired blood circulation in the lower extremities. Arterial wounds develop when blocked arteries reduce oxygen delivery to tissue — the underlying diagnosis is typically peripheral arterial disease (PAD). Venous wounds, including venous stasis ulcers, develop when failing venous valves allow blood to pool in the lower leg — the underlying diagnosis is typically chronic venous insufficiency (CVI). Each type requires a different treatment approach: arterial wounds are supported by arterial assist devices (E0675) that improve blood flow distally; venous wounds are treated with compression therapy and intermittent pneumatic compression devices (E0651/E0652) that augment venous return. Compression garments support both venous wound management and long-term prevention of recurrence. Getting the diagnosis right before beginning any device therapy is essential.
Vascular wounds and arterial wounds affect millions of Americans, yet the differences in how they form, how they're diagnosed, and how they're treated are widely misunderstood — even among patients who have been living with them for years. Whether your provider has mentioned peripheral arterial disease, chronic venous insufficiency, or simply described your wound as a circulation problem, what you do next matters enormously.
This guide explains the two primary categories of circulation-related wounds, how each is diagnosed, and why the right compression therapy or pneumatic compression device isn't just a comfort measure — it can be the difference between a wound that closes and one that doesn't.
If you've been referred to a DME supplier for a compression pump, a compression garment, or wound care support, understanding why your provider made that recommendation helps you use it correctly, consistently, and to the fullest benefit.

What Are Vascular Wounds — and Why Does the Type Matter?
The word "vascular" simply means related to blood vessels. In clinical practice, vascular wounds are chronic wounds — typically on the lower leg or foot — that develop because blood isn't moving the way it should. But that umbrella term covers two very different problems that require very different interventions.
Arterial wounds develop when the arteries carrying oxygenated blood to the tissues are narrowed or blocked. Without adequate oxygen delivery, tissue begins to break down. The underlying condition is typically peripheral arterial disease (PAD).
Venous wounds, including venous stasis ulcers, develop when the veins carrying blood back to the heart are failing. Blood pools in the lower extremity, pressure builds, and the surrounding skin and tissue eventually break down. The underlying condition is typically chronic venous insufficiency (CVI).
Getting the diagnosis right is the starting point for everything. Compression therapy is not suitable for people with peripheral artery disease, as it can affect the arterial blood supply. The device indicated for arterial insufficiency serves an entirely different physiologic purpose than a pneumatic compression pump for venous return. This is precisely why a thorough vascular assessment — and a prescription from a qualified provider — must come before any device is fitted.
Understanding Arterial Wounds and Peripheral Arterial Disease
What Causes Arterial Wounds?
Peripheral artery disease is a common condition caused by narrowing or blockage of the arteries, resulting in reduced blood supply. In the lower extremities, this means the feet and lower legs may not receive adequate oxygenated blood to sustain healthy tissue. When minor trauma occurs — a small cut, a pressure point from footwear, or a skin crack — the tissue cannot heal normally because the raw materials for repair aren't arriving in sufficient quantity.
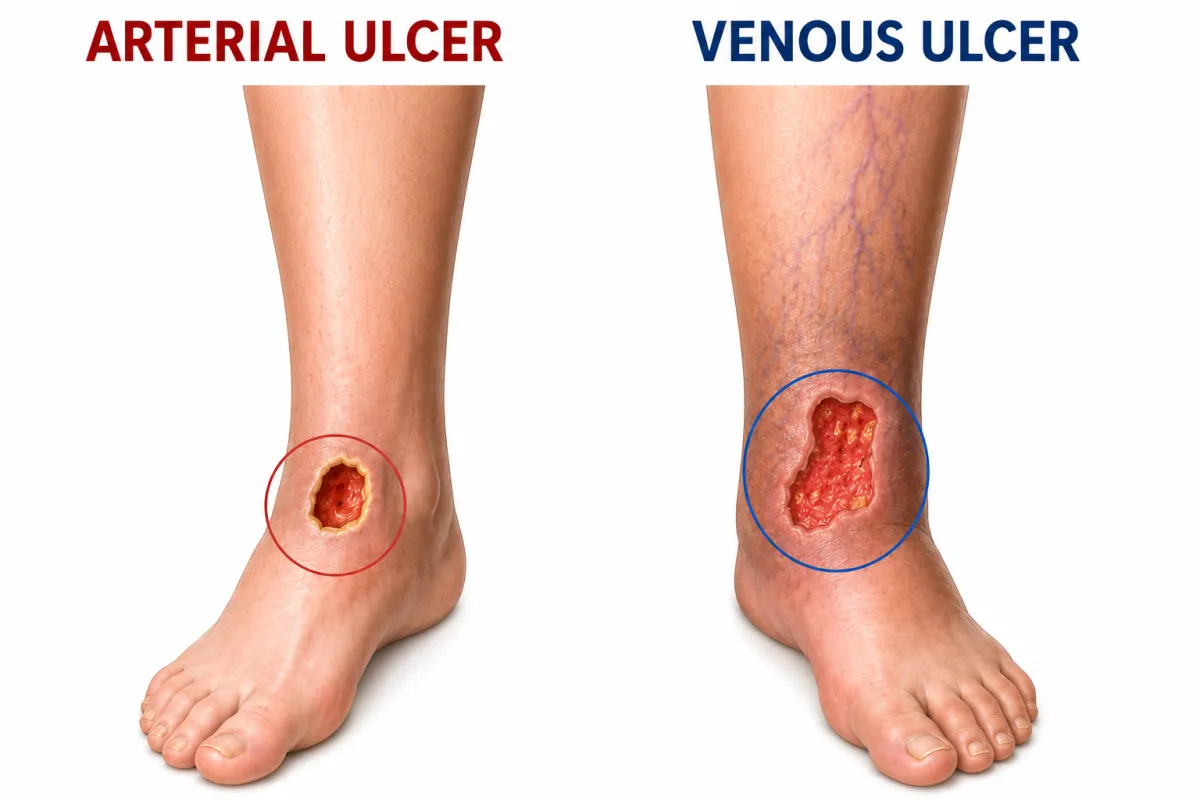
Arterial ulcers typically appear on the toes, the tops of the feet, or the lower shin. They tend to be small, deep, and well-defined with a "punched out" appearance. Unlike venous ulcers, they are often very painful, particularly when the leg is elevated or during rest. Patients frequently describe hanging a leg off the side of the bed at night to relieve pain — gravity temporarily improves perfusion to the foot.
Who Is at Risk for Arterial Wounds?
Smokers (the single strongest modifiable risk factor)
People with diabetes mellitus
Individuals with hypertension or high cholesterol
Adults over 65
Anyone with a history of cardiovascular disease or stroke
Diagnosing PAD: The Ankle-Brachial Index
In clinical practice, peripheral artery disease is identified by measurement of the ankle-brachial pressure index using a sphygmomanometer and manual Doppler device. The ABI compares blood pressure at the ankle to blood pressure at the arm. A reading below 0.9 typically indicates significant arterial disease; below 0.5 suggests severe ischemia warranting urgent vascular intervention.
When ABI readings are unreliable — as they often are in diabetic patients with arterial calcification — providers may order additional vascular imaging such as duplex ultrasound or toe-brachial pressure index testing.
How Arterial Assist Devices Support Wound Healing in PAD
The standard treatment for arterial wounds centers on restoring blood flow through medications, endovascular procedures, or surgery. For patients who are not candidates for revascularization — or who are awaiting intervention — the pneumatic arterial assist device (HCPCS code E0675) plays a meaningful role in augmenting distal perfusion.
The arterial assist device is designed to combat poor blood circulation in the arteries, aiming to enhance blood flow, reduce pain, and prevent complications associated with arterial insufficiency such as tissue damage and ulcers. The E0675 device uses a high-pressure, rapid inflation-and-deflation cycle — quite different from the slower sequential compression used in venous or lymphedema therapy. The rapid deflation creates a momentary drop in vascular resistance, pulling arterial blood distally into the foot and lower leg. Over multiple daily treatment sessions, this augmented perfusion supports tissue oxygenation and creates an environment more conducive to wound healing.
Learn more about arterial compression therapy and the E0675 device and how MCB DME supports patients and referring providers with this specialized equipment.
Understanding Venous Wounds and Chronic Venous Insufficiency
What Causes Venous Stasis Ulcers?
Venous insufficiency is a condition in which the flow of superficial or deep venous blood is impaired, causing venous hypertension. Chronic venous insufficiency encompasses several pathological changes — including lower extremity edema, skin trophic changes, cramping, and wounds — that result secondary to venous hypertension.
Healthy veins in the leg contain one-way valves that prevent blood from flowing backward between heartbeats. When those valves are damaged — through deep vein thrombosis, prolonged standing, obesity, or age — blood refluxes downward rather than returning efficiently to the heart. The result is sustained elevated pressure in the veins of the lower leg: ambulatory venous hypertension.
Over time, this leads to a cascade of physiological and histologic abnormalities including blood pooling, hypoxia, inflammation, swelling, skin changes such as lipodermatosclerosis, and in severe cases, venous leg ulcers. Venous leg ulcers represent up to 80% of all leg ulcers and have a prevalence of approximately 1% in the general population, with that prevalence increasing significantly with age.
Who Is at Risk for Venous Wounds?
In the United States, more than 25 million adults experience chronic venous insufficiency. Risk factors include age, family history, female sex, obesity, prolonged standing, pregnancy, parity, and a history of deep vein thrombosis. Each year, approximately 150,000 new patients are diagnosed with CVI, and nearly $500 million is spent on the care of these patients annually.
What Venous Ulcers Look Like
Venous stasis ulcers typically appear on the inner ankle and lower leg — the "gaiter zone." They are shallow with irregular borders, often surrounded by skin that is discolored bronze or brown from hemosiderin deposits. The wound bed is usually moist, and surrounding skin may appear thickened or hardened — signs of chronic lipodermatosclerosis. Unlike arterial ulcers, venous wounds tend to improve with leg elevation and worsen when the leg hangs down.

How Compression Therapy Treats Venous Wounds
Why Compression Is the Cornerstone of Venous Wound Care
Compression therapy addresses the root cause of venous ulceration: elevated venous pressure in the lower leg. By applying sustained, graduated external pressure, compression counteracts the venous hypertension that drives ulcer formation and impedes healing.
Comprehensive care of chronic venous insufficiency and associated ulcers requires a multipronged and interprofessional approach, including exercise, nutritional assessment, compression therapy, vascular reconstruction, and advanced treatment modalities.
Compression for venous wounds takes several forms:
Compression wraps and multi-layer bandaging systems apply sustained pressure around the clock. They require skilled application and are typically managed during the active wound-healing phase, often by wound care nurses or trained clinicians.
Medical-grade graduated compression garments — stockings, sleeves, or wraps — are the primary maintenance tool once a venous ulcer closes, or for patients managing early-to-moderate CVI before ulceration develops. Garments must be properly fitted: too little compression fails to counteract venous hypertension; too much may be poorly tolerated and reduce compliance.
Explore compression garments and wraps available through MCB DME for both active venous wound management and long-term prevention.
How Pneumatic Compression Devices Accelerate Venous Wound Healing
Beyond passive compression garments, intermittent pneumatic compression (IPC) devices provide active, rhythmic pressure that dynamically augments venous return and lymphatic drainage — and the clinical evidence supporting their use in venous wounds is compelling.
A landmark randomized controlled trial conducted at Rutgers New Jersey Medical School enrolled 52 patients with hard-to-heal venous ulcers averaging more than one year in duration and 31 cm² in surface area. The median time to wound closure was 141 days for the intermittent pneumatic compression–treated group versus 211 days for the compression bandaging–only control group. The healing rate was 0.8 mm/day for the control group and 2.1 mm/day for the IPC-treated group — more than double the healing rate in one of the most difficult-to-treat ulcer populations studied.
In a separate trial of 80 patients, more ulcers healed with IPC than with wound dressings alone — 62% versus 28%. The mechanism is multifactorial: IPC devices reduce chronic edema that impairs oxygen and nutrient delivery to the wound bed, augment venous return to reduce the hypertension that perpetuates ulceration, promote lymphatic flow to reduce inflammation, and stimulate endogenous fibrinolytic factors that combat the microthrombi associated with chronic venous disease.
Intermittent pneumatic compression should be considered a key front-line treatment for applying active compression to immobile limbs — to reduce edema, promote venous blood flow, and help expedite venous ulcer healing.
For patients with limited mobility who struggle with bandaging compliance, or whose wounds have failed to respond to bandaging alone, IPC represents a particularly important option — one that can be used safely at home without a clinician present for each session.
Learn more about lymphedema and venous compression pump options at MCB DME.
When Both Conditions Are Present: Mixed Arterial-Venous Disease
Some patients have elements of both arterial insufficiency and chronic venous insufficiency simultaneously — more common than many realize, particularly in older adults with multiple cardiovascular risk factors.
Mixed arterial-venous disease complicates treatment decisions significantly. Compression appropriate for a pure venous wound may be harmful if significant arterial disease is also present. Neglecting the venous component, however, allows ongoing wound expansion and infection risk.
Management of mixed disease requires vascular medicine or vascular surgery consultation. An individualized treatment plan guided by ABI values and duplex ultrasound findings is essential. In some cases, modified compression at lower pressure levels is safe. In others, arterial revascularization must precede any compression intervention.
If your wound care provider has not performed or ordered an ABI assessment, ask for one. It is the foundational piece of information that determines the safe path forward. The Society for Vascular Surgery provides patient-facing resources on vascular evaluation and when to seek specialist referral.

Expert Perspective: What Clinicians See in Practice
Several patterns emerge consistently in patients with chronic vascular wounds:
Delayed diagnosis is common. Many patients attribute leg swelling, skin changes, and fatigue to aging for months or years before a wound develops. By the time an ulcer appears, significant underlying disease has often been present for a long time. Earlier evaluation means earlier intervention — before a wound opens.
Device compliance determines outcomes. Whether the prescribed therapy is a compression stocking, a multi-layer bandage, or an IPC pump, patients who use their therapy consistently heal faster and recur less often. Inconsistent use of a compression garment is one of the most common reasons a healed venous ulcer reopens.
Compression garments must be replaced regularly. Graduated compression stockings lose their therapeutic pressure with washing and wear. Most garments should be replaced every three to six months to maintain clinically effective pressure gradients.
Not all pumps are the same. The lymphedema and venous IPC pump (E0651/E0652) and the arterial assist device (E0675) look similar but serve entirely different physiologic purposes. The wrong device in the wrong clinical context is ineffective at best and potentially harmful. Prescription specificity matters.
Local supply chains matter for wound care patients. Patients managing non-healing wounds often need timely equipment adjustments, garment replacements, or clinical follow-up. A DME supplier with local inventory — rather than national shipping — reduces the care gaps that allow wounds to deteriorate. MCB DME maintains inventory in Hawthorne, NJ and works closely with wound care teams across northern New Jersey.
Common Mistakes and Misconceptions About Vascular Wound Care
"My wound just needs better dressing." Wound dressings manage the surface — they do not address the underlying cause. A venous ulcer dressed without compression will rarely close permanently. An arterial ulcer managed without addressing perfusion will not heal regardless of the dressing used.
"Compression will make my leg feel worse." Properly fitted compression initially feels unfamiliar, but it should not cause pain in a patient without significant arterial disease. Pain or numbness with compression warrants an immediate reassessment and ABI check — but mild tightness is normal and expected as edema resolves.
"My swelling isn't that bad yet." Venous insufficiency is progressive. Approximately 25% of venous leg ulcers do not heal, and venous leg ulcers are the most common chronic leg ulcers in the geriatric population. Beginning compression before ulceration occurs is far more effective than trying to close a wound that has been open for months.
"I only need the pump when my leg looks swollen." Pneumatic compression devices deliver the most benefit when used consistently — typically once or twice daily as prescribed. Sporadic use fails to maintain the venous return and edema-reduction benefits that move wounds toward closure.
"Once my wound closes, I'm done." Venous ulcer recurrence rates remain high without ongoing maintenance compression. Most patients with a history of venous ulceration require long-term compression garment use to prevent reopening.
When to Seek Specialized Wound Care or a Vascular Referral
Contact your primary care provider, wound care specialist, or vascular physician promptly if you notice:
A wound that has not improved meaningfully after four weeks of appropriate treatment
Signs of infection: increasing redness, warmth, drainage, or fever
A wound that has been present for more than three months without closure
Sudden or significant increase in leg pain, particularly at rest or with leg elevation
Darkening or blackening of tissue at wound edges
Any new wound on a foot or leg in a patient with known PAD or diabetes
Early vascular consultation changes outcomes. The Association for the Advancement of Wound Care and the American Venous Forum provide evidence-based clinical guidelines supporting an interprofessional approach to chronic wound management — one that typically includes wound care nursing, vascular surgery, and DME providers working in coordination.
For patients receiving a new DME prescription for a compression device or pump, working with a Medicare-enrolled DMEPOS supplier who specializes in vascular care ensures that fitting, documentation, and ongoing support are handled by people who understand the clinical context. Visit our patients page or contact us to get started.
FAQ: Vascular Wounds, Arterial Wounds, and Compression Therapy
What is the difference between an arterial wound and a venous wound?
Arterial wounds result from insufficient oxygenated blood reaching the tissues — most commonly from peripheral arterial disease (PAD). They typically appear on the toes or foot and are painful at rest. Venous wounds result from failed venous valves that cause blood to pool in the lower leg, creating chronic pressure that breaks down surrounding tissue. They typically appear on the inner ankle and worsen with prolonged standing or sitting. Each requires different diagnosis, devices, and treatment.
Can compression therapy be used for arterial wounds?
Standard compression therapy is generally contraindicated in significant arterial disease because it can further restrict already-compromised blood flow. The appropriate device for arterial wounds is the arterial assist device (E0675), which improves distal perfusion rather than applying sustained external pressure. Patients with mixed arterial-venous disease require individual evaluation by a vascular specialist.
What is an arterial assist device and how does it help wounds?
The arterial assist device (HCPCS E0675) uses a high-pressure, rapid inflation-deflation cycle to augment arterial blood flow to the foot and lower leg. By improving tissue perfusion, it supports oxygenation and wound healing in PAD patients who are not yet candidates for — or who are awaiting — revascularization procedures.
How does a pneumatic compression pump help venous ulcers?
Intermittent pneumatic compression (IPC) devices improve venous return, reduce chronic edema, and support lymphatic drainage. A randomized controlled trial at Rutgers New Jersey Medical School found IPC more than doubled healing rates in hard-to-heal venous ulcers — 2.1 mm/day versus 0.8 mm/day — compared to compression bandaging alone.
How long does it take for a venous ulcer to heal with compression therapy?
Healing time varies based on wound size, duration, and treatment consistency. The Rutgers NJ Medical School trial found a median closure time of 141 days with IPC plus compression, versus 211 days with compression bandaging alone. Some patients with smaller wounds caught earlier close within four to eight weeks with consistent treatment.
Is a prescription required for a compression pump or compression garments?
Yes. Medicare-covered compression devices and medical-grade compression garments require a physician prescription and supporting clinical documentation, including diagnosis codes and relevant vascular assessments. A Medicare-enrolled DMEPOS supplier ensures the ordering process meets coverage requirements.
What is the difference between a lymphedema/venous pump and an arterial pump?
Despite similar appearance, these devices serve entirely different purposes. IPC devices for lymphedema and venous indications (E0651/E0652) use sequential gradient compression to move excess fluid proximally and augment venous return. Arterial assist devices (E0675) use high-pressure rapid cycles to push oxygenated blood distally into the foot. Using the wrong device in the wrong clinical context is both ineffective and potentially unsafe.
Key Takeaways
Vascular wounds divide into two primary categories — arterial and venous — with different causes, presentations, and required treatments. Accurate diagnosis drives everything downstream.
Peripheral arterial disease (PAD) causes arterial wounds by reducing oxygen delivery to the tissues. The ankle-brachial index (ABI) is the standard diagnostic screening tool.
Chronic venous insufficiency (CVI) causes venous stasis ulcers by allowing blood to pool in the lower leg, creating sustained venous hypertension that breaks down surrounding tissue over time.
Standard compression therapy is the cornerstone of venous wound treatment but is contraindicated in significant arterial disease. An ABI assessment must precede any compression prescription.
Arterial assist devices (E0675) augment distal blood flow in PAD patients, supporting wound healing and reducing ischemic pain in patients not yet eligible for revascularization.
Intermittent pneumatic compression devices (E0651/E0652) significantly improve healing rates in venous wounds — more than doubling healing speed in clinical trials when combined with compression bandaging.
Compliance with prescribed therapy — garment, bandage, or pump — is one of the strongest predictors of wound closure and recurrence prevention.
Mixed arterial-venous disease requires specialized vascular evaluation before any compression intervention is initiated.
Take the Next Step
For patients: If you've been diagnosed with PAD, chronic venous insufficiency, or a non-healing wound, the right compression device or pump — properly fitted and Medicare-covered — can meaningfully change your outcome. Contact us to connect with our team, or explore our arterial therapy and compression therapy pages to learn what's available.
For referring providers: MCB DME supports vascular wound patients with arterial assist devices, lymphedema and venous IPC pumps, and compression garment fittings across northern New Jersey. Visit our providers page for referral documentation support and coverage guidance.
Related Reading
Medical Disclaimer: This article is intended for educational purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. Compression therapy and pneumatic compression devices carry clinical indications and contraindications that must be evaluated by a qualified healthcare provider. Always consult your physician, wound care specialist, or vascular surgeon before beginning any compression or device therapy.
